What Is Alopecia Areata?
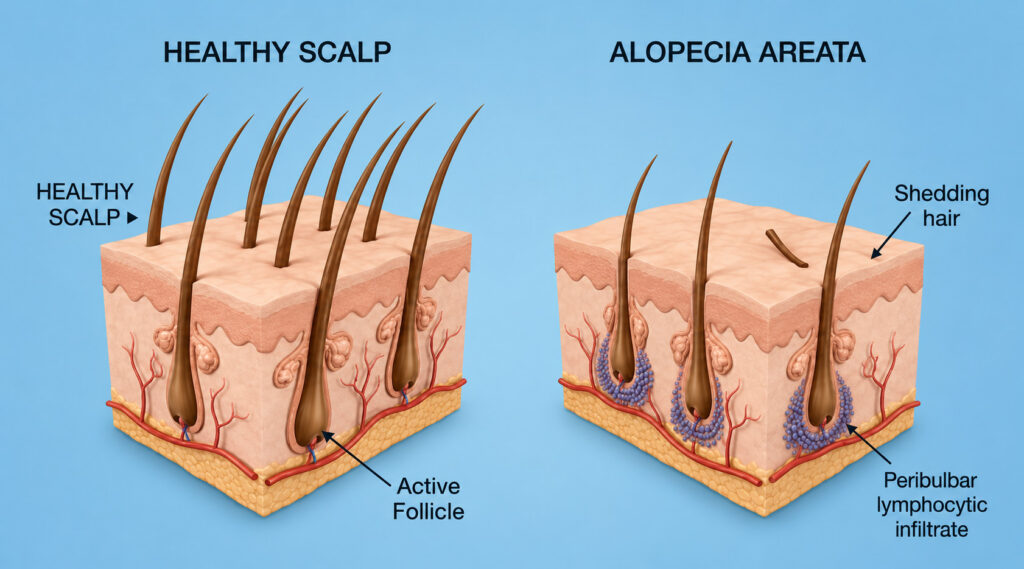
Alopecia areata is an autoimmune condition in which the body’s immune system mistakenly attacks hair follicles, causing hair loss. The critical distinction from scarring alopecia is that the follicle itself is not destroyed — it is suppressed. The immune attack puts the follicle into a state of dormancy, halting hair production. This means that the biological machinery for hair growth remains intact, and regrowth is possible when the immune assault is controlled.
This is simultaneously the most hopeful and the most frustrating aspect of alopecia areata: the potential for complete regrowth exists, but the disease is unpredictable. Some patients experience a single episode that is resolved spontaneously. Others have chronic, relapsing courses. A subset progress to extensive or total hair loss that can be profoundly life-altering.

Before and 6 months after medical treatment with intralesional Kenalog and topical minoxidil.
The Clinical Spectrum - Alopecia areata exists on a spectrum of severity.
Patchy alopecia areata is the most common presentation: one or several smooth, round, well-demarcated patches of hair loss, typically on the scalp. The skin in these patches appears normal — no redness, scaling, or scarring — which helps distinguish it from other causes of patchy hair loss.
Alopecia totalis refers to the complete loss of all scalp hair. Alopecia universalis refers to loss of all body hair, including eyebrows, eyelashes, nasal hair, and body hair. These represent the severe end of the spectrum and affect a smaller proportion of patients.
Ophiasis is a pattern in which hair loss occurs in a band-like distribution around the occipital and temporal scalp margins. This pattern tends to be more treatment-resistant and carries a more guarded prognosis than classic patchy disease.
Nail changes — including pitting, ridging, brittleness, and trachyonychia (rough, sandpaper-like nails) — are present in a subset of patients and can be a marker of more extensive disease.
What Causes the Immune Attack?
Under normal conditions, the hair follicle enjoys a state of “immune privilege” — it actively suppresses immune surveillance in its immediate environment, preventing the immune system from recognizing and attacking follicular cells. In alopecia areata, this immune privilege collapses. The follicle begins presenting self-antigens to circulating T-lymphocytes, which then mount an inflammatory attack concentrated at the hair bulb.
The triggers for this collapse are not fully understood. Genetic predisposition plays a significant role — patients with alopecia areata have a higher prevalence of other autoimmune conditions, including autoimmune thyroid disease, vitiligo, and type 1 diabetes, and the condition runs in families. Physiologic stress (emotional, surgical, infectious) can serve as a precipitating event, and COVID-19 has been linked to new-onset alopecia areata in a number of published case series, though the exact relationship remains under investigation.
Not everyone with alopecia areata will have an identifiable trigger. For many patients, the onset is seemingly spontaneous.
Prognostic Factors
Being honest about prognosis is essential for building trust and setting realistic expectations:
Favorable factors: Limited patchy disease (one to a few small patches), onset in adulthood, short duration of current episode, no nail involvement, and no personal or family history of autoimmune disease. The majority of patients with limited patchy alopecia areata experience spontaneous regrowth within 6–12 months.
Less favorable factors: Extensive disease (more than 50% scalp involvement), early age of onset (particularly childhood), ophiasis pattern, prolonged duration (years without regrowth), nail changes, and concurrent autoimmune conditions. Patients with alopecia totalis or universalis that has been present for years face a more guarded prognosis, though the advent of JAK inhibitors has opened new possibilities even for these patients.

Alopecia areata of the eyebrow before and after treatment with compounded topical minoxidil, topical jak inhibitor, and topical bimatoprost.
Treatment Landscape
Intralesional Corticosteroids: The Workhorse for Limited Disease
For patients with one to several patches of alopecia areata, intralesional injection of triamcinolone acetonide (a corticosteroid) is the first-line treatment. Tiny amounts are injected directly into and around the patches every 4–8 weeks. This delivers a potent anti-inflammatory effect precisely where the immune attack is occurring, without significant systemic exposure.
Most patients with limited disease respond well to this approach, with regrowth typically visible within 4–8 weeks of the first treatment. The injections can be uncomfortable, but the procedure is quick and well-tolerated.
Topical Therapies
High-potency topical corticosteroids (such as clobetasol) can be used as an adjunct to injections or as primary therapy in patients who are averse to needles — particularly children. Topical minoxidil (5%) is often added to support regrowth, though it does not address the underlying immune process.

JAK Inhibitors: A Major Advance
The development of Janus kinase (JAK) inhibitors represents the most significant therapeutic advance in alopecia areata in decades. Baricitinib (Olumiant) was the first FDA-approved oral treatment for severe alopecia areata in adults, and ritlecitinib (Litfulo) has since been approved for patients 12 years and older.
These medications work by blocking the JAK-STAT signaling pathway — the specific intracellular cascade that drives the T-cell attack on the hair follicle. In clinical trials of baricitinib, approximately 40% of patients with severe alopecia areata (80% or more scalp hair loss at baseline) achieved 80% or greater hair regrowth at the 4 mg dose over 36 weeks.
The practical realities: JAK inhibitors work while you take them. Discontinuation frequently leads to relapse — the disease recurs because the underlying autoimmune tendency has not been eliminated, only suppressed. This means patients may need to take these medications long-term, which raises cost and monitoring considerations. JAK inhibitors carry risks including increased susceptibility to infections, potential cardiovascular and malignancy concerns (based on data from the rheumatology population), and laboratory changes that require periodic monitoring. These risks must be weighed against the benefit, and the decision should be made collaboratively between patient and physician.
Insurance coverage for JAK inhibitors varies and can be a significant barrier. Prior authorization, appeals, and manufacturer assistance programs may be necessary.
An emerging approach that has shown promising results is combining JAK inhibitors with oral minoxidil. Small studies have demonstrated that this combination produces regrowth in roughly two-thirds of patients — a higher response rate than JAK inhibitors alone. The rationale is straightforward: the JAK inhibitor suppresses the immune attack, while minoxidil directly stimulates follicular growth. Together, they address both sides of the problem simultaneously.
Topical Immunotherapy
For patients with extensive disease who are not candidates for or prefer to avoid systemic therapy, topical immunotherapy with diphenylcyclopropenone (DPCP) or squaric acid dibutyl ester (SADBE) is an option. These are contact sensitizers that are applied to the scalp to provoke a controlled allergic response, which is thought to redirect the immune system’s attention away from the hair follicle. The treatment requires weekly in-office application and takes months to show effect, but it can produce meaningful regrowth in some patients.
Systemic Steroids
Short courses of systemic corticosteroids (pulsed oral dexamethasone or oral prednisone) can halt rapid progression of alopecia areata and provide a bridge to longer-term therapy. They are not a sustainable long-term solution due to the well-known side effects of chronic steroid use, but they can be valuable in acute, rapidly progressing disease.
Emerging Research and Future Directions
The treatment landscape for alopecia areata is evolving rapidly. Several new JAK inhibitors are in clinical trials, and topical JAK inhibitor formulations are under development that may provide localized immune modulation with fewer systemic effects. Research into the mechanisms of follicular immune privilege is also advancing, with the hope that future therapies may restore immune privilege rather than suppress the immune system broadly.
Other investigational approaches include targeted biologic therapies, small-molecule inhibitors of additional inflammatory pathways, and combination protocols designed to achieve sustained remission after discontinuation. While these are not yet available in clinical practice, they represent a pipeline of options that may significantly expand the treatment toolkit in the coming years.
The Psychological Impact
Alopecia areata can be profoundly distressing, particularly in its more severe forms. Hair loss that is sudden, unpredictable, and visible affects self-image, social confidence, and quality of life. Children and adolescents may be especially vulnerable to bullying and social isolation.
Acknowledging this impact is important, but so is providing the clinical structure to address it: an accurate diagnosis, a rational treatment plan, and honest communication about prognosis. The National Alopecia Areata Foundation (NAAF) provides peer support resources, educational materials, and clinical trial information that many patients find valuable.
Why See a Dermatologist?
Alopecia areata management requires understanding the immune mechanism at play, distinguishing it from mimics (tinea capitis, trichotillomania, secondary syphilis, early scarring alopecia), and managing the potential side effects of systemic immunologic therapy. These are core dermatologic competencies.

Tinea capitis — a fungal scalp infection — can closely mimic patchy alopecia areata, particularly in children, and requires antifungal treatment rather than immunosuppression. Trichotillomania (compulsive hair pulling) produces irregularly shaped patches with broken hairs of varying lengths, a pattern that can overlap with AA on first glance. Secondary syphilis can cause a “moth-eaten” alopecia pattern that requires entirely different treatment. A trained dermatologist can efficiently distinguish these conditions, often with a single clinical encounter and targeted testing.
Additionally, for patients who achieve disease stability and desire surgical restoration of areas that have not regrown, having a dermatologist who also performs hair transplantation means the patient does not need to be referred to a separate surgical practice.
A Personal Connection
Alopecia areata is personal to Dr. Hawkins. During his dermatology residency, his wife suffered a severe case of alopecia areata. Watching her navigate the emotional and clinical challenges of the disease firsthand — the unpredictability, the difficulty finding providers who truly understood the condition, the impact on daily life — was the experience that inspired him to learn everything he could about hair loss. That commitment ultimately led to his ISHRS fellowship in hair restoration surgery and motivated the founding of the Hair Medicine Institute.
This background shapes the care that AA patients receive at HMI. It means a physician who understands the condition not just clinically but personally, who takes the emotional toll seriously without making it the entire conversation, and who is invested in staying at the leading edge of the treatment landscape because this disease is not abstract to him.

Next Steps
If you have developed one or more patches of smooth hair loss — or are experiencing widespread shedding that may indicate a more extensive form of alopecia areata — a comprehensive evaluation by a board-certified dermatologist is the essential first step. The treatment landscape for alopecia areata has evolved significantly in recent years, and for many patients, meaningful regrowth is achievable with the right approach. At Hair Medicine Institute, Dr. Hawkins provides expert diagnosis, a full range of medical treatments including JAK inhibitors and combination protocols, and surgical restoration for patients with stable disease.
Without Treatment,
Your Hair Loss Will Continue.
Get a personalized treatment plan and get your hair back.