Hair Loss Stops Here.
Get long-lasting results from medical therapy and transplantation.

What Is Androgenetic Alopecia?
Androgenetic alopecia — commonly called male pattern baldness — is the most common cause of hair loss in men, affecting roughly 50% of men by age 50 and an even greater proportion by age 70. Despite its prevalence, it remains widely misunderstood. This is not simply “genetics” in the vague sense most people mean. It is a specific, well-characterized process in which the hormone dihydrotestosterone (DHT) progressively shrinks genetically susceptible hair follicles until they can no longer produce visible hair.

DHT is produced from testosterone by an enzyme called 5-alpha reductase, which is active at the level of the hair follicle. Follicles in the frontal, temporal, and vertex regions of the scalp express high densities of androgen receptors, making them vulnerable to DHT-mediated miniaturization. With each successive hair cycle, the growth phase (anagen) shortens, and the hair produced becomes thinner, shorter, and less pigmented — until eventually the follicle produces only a fine, nearly invisible vellus hair, or stops producing hair altogether.
Follicles on the back and sides of the scalp have far fewer androgen receptors and are largely resistant to this process. This biological fact is what makes hair transplantation possible: hairs moved from the resistant “safe donor zone” to the affected areas retain their DHT resistance permanently.
Recognizing the Pattern
Male pattern hair loss follows predictable trajectories classified by the Norwood scale. Understanding where you fall helps frame both the urgency and the treatment approach.
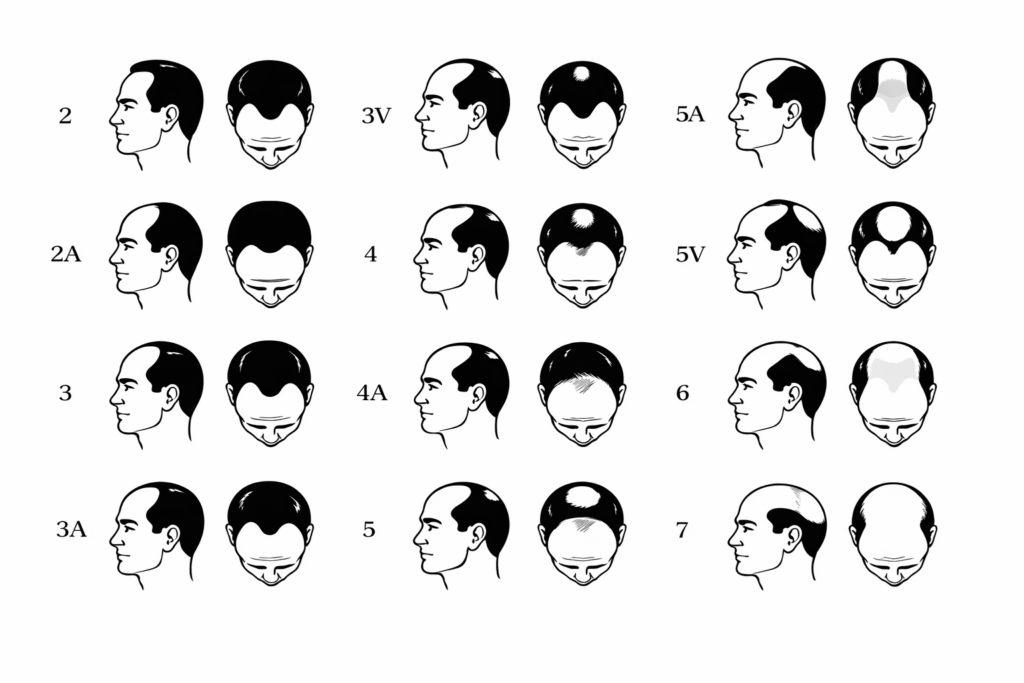
The Norwood Hair Loss Scale
Early stages (Norwood II–III): Temporal recession begins — the hairline moves backward at the corners, creating an “M” shape. Hair at the frontal midline may still be intact. Many men notice this in their mid-twenties to early thirties. This is the ideal window for medical therapy. The follicles are miniaturizing but not yet lost, and aggressive treatment can stabilize or partially reverse the process.
Intermediate stages (Norwood III vertex–IV): Thinning at the crown becomes noticeable, and the frontal recession deepens. The bridge of hair connecting the front to the crown begins to thin. Medical therapy remains critical, and this is often the stage where patients begin considering transplantation to restore density in areas that have not responded to medication.
Advanced stages (Norwood V–VII): The frontal and vertex zones merge into a single large area of loss, with hair remaining only on the sides and back. At this point, the available donor supply must be carefully budgeted. Medical therapy is still valuable for preserving what remains, but surgical planning becomes more strategic and expectations must be calibrated.
Why Doing Nothing Is Itself a Decision
Androgenetic alopecia is progressive. Without intervention, it continues to advance. There is no stage at which it spontaneously stabilizes, and the follicles that are lost to miniaturization become increasingly difficult — and eventually impossible — to recover. The most common regret expressed by patients is waiting too long to start treatment. Every month of delay means more follicles that have crossed from “treatable” to “lost.”
This does not mean that every man who notices slight temple recession needs to start medication immediately. But it does mean that anyone who is bothered by their hair loss, or who anticipates being bothered as it progresses, should at a minimum get a baseline evaluation. Hence, they understand the trajectory and can make an informed decision about timing.

Don’t Let Hair Loss Hold You Back
At a certain point in life, you realize you are successful. You've built a good life. Why are you letting your hair hold you back?
You deserve to look your best.
At Hair Medicine Institute, we know hair loss can leave you feeling frustrated, older, unsure, maybe even a little depressed.
YOU ARE NOT ALONE.

of men view hair as a crucial aspect of their self-image.

of men believe that hair loss negatively impacts their self-esteem.

of men associate hair loss with feeling older.

THE RIGHT SOLUTION
When it comes to hair restoration, there is a lot of conflicting information.
It's hard to know what to trust.
You need someone medically qualified who can help you navigate complex treatment options and find the right long-term
term solution for you.
That's what we do.
Hair restoration is not a one-size-fits-all solution. What works for one person may not be right for you.
Learn More About Hair Loss
Medical Therapy: The Foundation
DHT-Blocking Therapy
The cornerstone of medical treatment for androgenetic alopecia is blocking DHT — the hormone driving follicular miniaturization. Two medications accomplish this: finasteride and dutasteride. Both inhibit 5-alpha reductase, the enzyme that converts testosterone to DHT, but they differ in scope. Finasteride (1 mg) blocks only the Type II isoform, reducing DHT by approximately 70%. Dutasteride (0.5 mg) blocks both Type I and Type II, reducing DHT by approximately 90%. Head-to-head studies consistently show that dutasteride is more effective.
 The choice between them depends on where you are in life. For men in their twenties and thirties who have not yet finished having children, we tend to start with finasteride. It has a short half-life (6–8 hours, cleared in 1–2 days) and does not decrease sperm counts at the standard 1 mg dose. Dutasteride has a half-life of approximately 5 weeks and may slightly lower sperm counts, making it less ideal for men still planning a family. Once a man is done having children, we often transition to oral dutasteride for more comprehensive DHT suppression.
The choice between them depends on where you are in life. For men in their twenties and thirties who have not yet finished having children, we tend to start with finasteride. It has a short half-life (6–8 hours, cleared in 1–2 days) and does not decrease sperm counts at the standard 1 mg dose. Dutasteride has a half-life of approximately 5 weeks and may slightly lower sperm counts, making it less ideal for men still planning a family. Once a man is done having children, we often transition to oral dutasteride for more comprehensive DHT suppression.
For younger men seeking more aggressive treatment without the systemic profile of oral dutasteride, there is an effective middle ground: topical dutasteride applied to the scalp, combined with oral finasteride. This delivers more potent DHT suppression at the follicular level while keeping systemic exposure lower than oral dutasteride alone.
Sexual side effects — decreased libido, erectile dysfunction — occur in approximately 2% of men taking oral finasteride and approximately 4% with oral dutasteride. These are reversible with discontinuation in the vast majority of cases. For patients who want to avoid any systemic sexual side-effect risk entirely, topical clascoterone blocks DHT at the follicle without reducing circulating hormone levels.
Oral Minoxidil
Low-dose oral minoxidil (typically 2.5–5 mg daily for men) complements DHT-blocking therapy by working through a different mechanism. Minoxidil prolongs the anagen (growth) phase and enhances blood flow and nutrient delivery to the follicle via vasodilation and direct stimulation of dermal papilla cells. It was originally a blood pressure medication, and at the low doses used for hair loss, it rarely has clinically significant effects on blood pressure.
Oral minoxidil is more effective than topical formulations — studies comparing twice-daily topical to once-daily oral show higher hair counts with the oral form — and most patients find it far more convenient. The most common side effect is hypertrichosis (increased body and facial hair), which is dose-dependent and reversible. Minoxidil is not associated with sexual side effects.
Custom Compounding
At HMI, we frequently use custom compounding to simplify treatment regimens. This includes both oral and topical formulations. A single all-in-one oral capsule combining minoxidil with dutasteride (or finasteride) can reduce daily pill burden to one medication. On the topical side, compounded solutions can deliver higher-concentration minoxidil (5–8%) combined with finasteride or dutasteride directly to the scalp, reducing systemic exposure while providing meaningful DHT reduction at the follicular level.
Regenerative Therapy: Augmenting the Foundation
Medical therapy is the foundation, but regenerative interventions can enhance and accelerate results. At HMI, the baseline regenerative protocol uses a fractional non-ablative laser (Lumenis M22 ResurFX at 1565nm—the same wavelength as the FDA-cleared Folix system) to stimulate angiogenesis and create microchannels in the scalp, followed by ultrasound-enhanced delivery of the Xtressé FR peptide concentrate. For patients who want to be more aggressive, microneedling with Xvie exosomes or injectable PRP can be added. At home, the Revian Red LLLT cap (10 minutes daily, with physician-monitored compliance) provides an additional layer of daily follicular stimulation.
These treatments complement, but do not replace, consistent medical therapy. Patients who expect regenerative treatments to work as a standalone solution are generally disappointed; those who use them to augment a solid medication regimen see measurably better outcomes.
Don’t Ignore Your Hair Loss
All too often, men wait too long to address their hair loss. The earlier you address the signs, the more hair you can save.
If you don’t start treatment, your hair loss will continue.
Your hairline will noticeably continue to recede.
The balding on the crown of your head will continue to expand.
You might find your self-esteem waning, feeling more inclined to withdraw socially, and possibly see a dip in your performance at work.

Hair Transplantation: The Surgical Phase
Hair transplantation is the most reliable method for restoring hair to areas that are completely bald or unresponsive to medical therapy. At HMI, transplantation is positioned as Phase Three of the treatment plan — after medical therapy has stabilized the loss and the scalp environment has been optimized.

Recipient area with hairline marked out and donor area after FUE harvest.
Two techniques are available: FUE (follicular unit excision), in which individual grafts are extracted one by one using a sub-millimeter punch tool, and FUT (follicular unit transplantation, or strip method), in which a strip of donor tissue is excised and dissected into individual grafts. Each has distinct advantages. FUE avoids a linear scar but requires shaving the donor area and yields approximately 6,000 lifetime grafts. FUT preserves more grafts from the ideal central donor zone (potentially 9,000+ lifetime grafts when combined with subsequent FUE), does not require shaving, and the resulting linear scar is effectively invisible in patients who wear their hair at any length beyond a close buzz.
The right technique depends on the patient’s degree of loss, hair characteristics, styling preferences, and anticipated future needs. A surgeon who can perform and counsel on both techniques — rather than defaulting to one — is essential for creating a long-term surgical plan. If your surgeon only offers FUE, get a second opinion.
Common Myths
“Hair loss comes from your mother’s side.” Androgenetic alopecia is polygenic — it involves multiple genes inherited from both parents. While the androgen receptor gene is on the X chromosome (inherited from the mother), other contributing genes are autosomal. Looking only at your maternal grandfather is an incomplete predictor.
“Finasteride will ruin your sex life.” The internet has amplified legitimate but statistically uncommon side effects into near-universal certainty. In controlled studies, the incidence of sexual side effects with finasteride is approximately 2% in the first year and drops below 1% with continued use. These effects are reversible with discontinuation. Many men have been frightened away from an effective, well-studied medication by anecdotal online accounts that do not reflect the clinical data.
“Just shave it — it’s the only real option.” Shaving is a perfectly valid personal choice, but it is not the only option, and framing it as such dismisses effective medical and surgical treatments that have decades of evidence behind them. If you want to treat your hair loss, real solutions exist.
“It’s too early to treat” or “It’s too late.” It is almost never too early to start monitoring and considering preventive therapy, and it is rarely too late to benefit from some form of treatment — medical, regenerative, or surgical. The optimal strategy depends on where you are now and where the trajectory is heading.
Next Steps
If you are noticing thinning at the temples, crown, or along your part — or if you have been watching your hair change for years and are ready to act — a comprehensive evaluation is the starting point. At Hair Medicine Institute, every consultation includes dermoscopic scalp analysis, a full medical and family history review, and a candid discussion about what is realistic for your specific pattern and goals. Dr. Hawkins is the only dermatologist in Georgia who is also fellowship-trained in hair restoration surgery, which means diagnosis and the full spectrum of treatment — medical, regenerative, and surgical — are available under one roof.

*All results at 6 months after commencement of combination medical therapy.
RESTORE YOUR HAIR LOSS
Stay on Top of Your Game.
Men trust our evidence-based medical approach for long-lasting hair restoration.
 Assess Your Hair Loss
Assess Your Hair Loss
Receive a personalized, comprehensive physician-tailored treatment plan specifically designed for your type of hair loss.
 Start Your Treatment
Start Your Treatment
You’ll be guided through your holistic treatment plan step-by-step by our dermatologist-led care team
 Get Long Lasting Results
Get Long Lasting Results
See results within 6 months and be supported long term for a lasting solution.


Without Treatment,
Your Hair Loss Will Continue.
Get a personalized treatment plan and get your hair back.