What Is Androgenetic Alopecia?
Androgenetic alopecia — commonly called male pattern baldness — is the most common cause of hair loss in men, affecting roughly 50% of men by age 50 and an even greater proportion by age 70. Despite its prevalence, it remains widely misunderstood. This is not simply “genetics” in the vague sense most people mean. It is a specific, well-characterized process in which the hormone dihydrotestosterone (DHT) progressively shrinks genetically susceptible hair follicles until they can no longer produce visible hair.
DHT is produced from testosterone by an enzyme called 5-alpha reductase, which is active at the level of the hair follicle. Follicles in the frontal, temporal, and vertex regions of the scalp express high densities of androgen receptors, making them vulnerable to DHT-mediated miniaturization. With each successive hair cycle, the growth phase (anagen) shortens, and the hair produced becomes thinner, shorter, and less pigmented — until eventually the follicle produces only a fine, nearly invisible vellus hair, or stops producing hair altogether.
Follicles on the back and sides of the scalp have far fewer androgen receptors and are largely resistant to this process. This biological fact is what makes hair transplantation possible: hairs moved from the resistant “safe donor zone” to the affected areas retain their DHT resistance permanently.
Recognizing the Pattern
Male pattern hair loss follows predictable trajectories classified by the Norwood scale. Understanding where you fall helps frame both the urgency and the treatment approach.
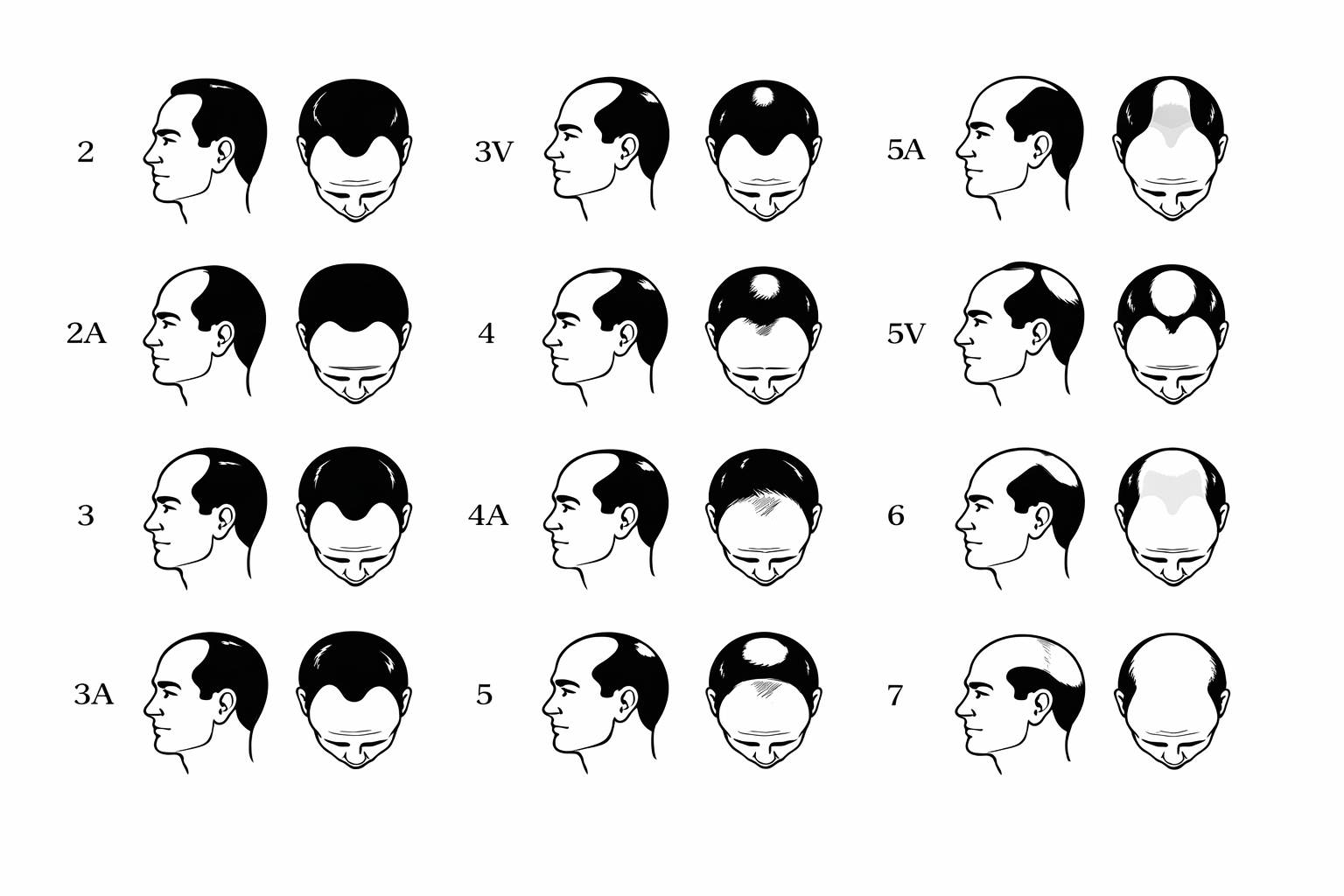
The Norwood Hair Loss Scale
Early stages (Norwood II–III): Temporal recession begins — the hairline moves backward at the corners, creating an “M” shape. Hair at the frontal midline may still be intact. Many men notice this in their mid-twenties to early thirties. This is the ideal window for medical therapy. The follicles are miniaturizing but not yet lost, and aggressive treatment can stabilize or partially reverse the process.
Intermediate stages (Norwood III vertex–IV): Thinning at the crown becomes noticeable, and the frontal recession deepens. The bridge of hair connecting the front to the crown begins to thin. Medical therapy remains critical, and this is often the stage where patients begin considering transplantation to restore density in areas that have not responded to medication.
Advanced stages (Norwood V–VII): The frontal and vertex zones merge into a single large area of loss, with hair remaining only on the sides and back. At this point, the available donor supply must be carefully budgeted. Medical therapy is still valuable for preserving what remains, but surgical planning becomes more strategic and expectations must be calibrated.
Why Doing Nothing Is Itself a Decision
Androgenetic alopecia is progressive. Without intervention, it continues to advance. There is no stage at which it spontaneously stabilizes, and the follicles that are lost to miniaturization become increasingly difficult — and eventually impossible — to recover. The most common regret expressed by patients is waiting too long to start treatment. Every month of delay means more follicles that have crossed from “treatable” to “lost.”
This does not mean that every man who notices slight temple recession needs to start medication immediately. But it does mean that anyone who is bothered by their hair loss, or who anticipates being bothered as it progresses, should at a minimum get a baseline evaluation. Hence, they understand the trajectory and can make an informed decision about timing.