Beyond Finasteride: What Comes Next When You Want More
For patients with androgenetic alopecia who are on finasteride and want to push their results further, the conventional next step has been clear for years: switch to dutasteride. The clinical trials supporting dutasteride's superiority over finasteride are real and consistent, and for many patients, this remains the right move.
But the conversation is more interesting than "more is better." Topical clascoterone — an FDA-approved androgen receptor antagonist — has emerged as a mechanistically distinct alternative that attacks the same biological problem from a different direction. For some patients, particularly younger men with concerns about systemic side effects or future fertility, the comparison between these two options deserves a more thoughtful conversation than the standard "just take dutasteride."

This post walks through how both options work, what the data show, and the trade-offs that should guide the decision for any given patient.
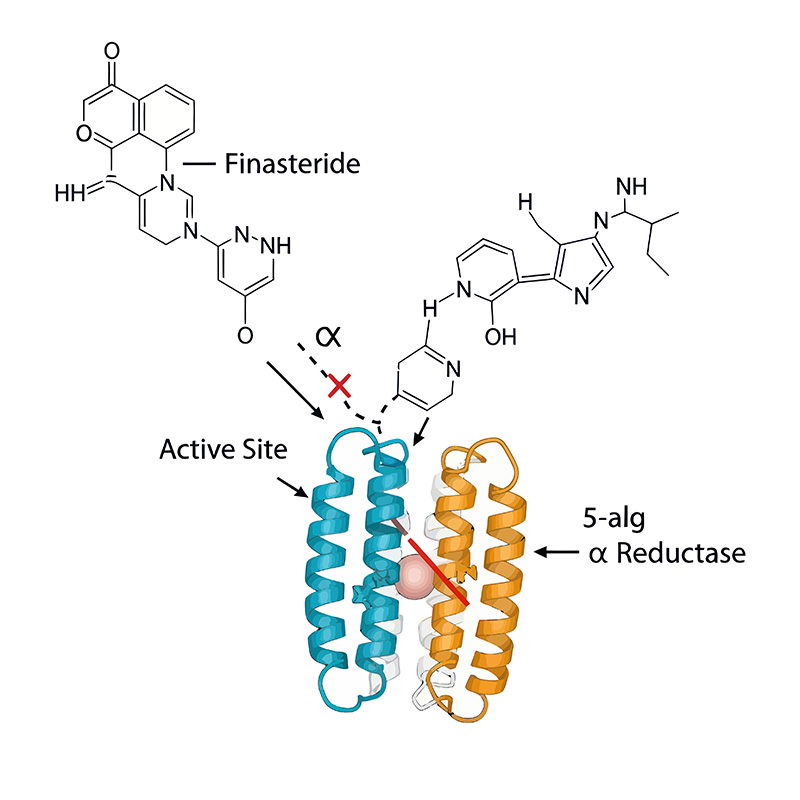
Finasteride 1 mg daily reduces serum DHT by approximately 70% by blocking the Type 2 isoform of 5-alpha reductase, the enzyme that converts testosterone to DHT. This is the foundational therapy for androgenetic alopecia in men, and it works — multiple decades of clinical data confirm its efficacy and acceptable safety profile.
At the scalp, where it matters for hair loss, finasteride reduces tissue DHT by approximately 50%. This is less than the serum reduction for an important reason: the scalp has substantial Type 1 5-alpha reductase activity, particularly in sebaceous glands and the outer root sheath of hair follicles. Finasteride only blocks Type 2, so the Type 1-generated DHT pool remains.
For patients who respond well to finasteride and achieve stabilization or improvement, no additional intervention may be needed. The question of what comes next applies to patients who have stabilized but want further density improvement, or who are continuing to progress despite consistent finasteride use.
Option one: switching to dutasteride
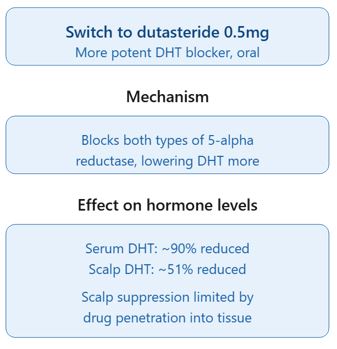
Dutasteride 0.5 mg daily blocks both Type 1 and Type 2 5-alpha reductase. The serum DHT reduction jumps to approximately 90% — a dramatic difference from finasteride's 70%.
The scalp data is more interesting, and worth understanding clearly. In the foundational dose-finding study by Olsen and colleagues, dutasteride at 0.5 mg suppressed scalp DHT by 51%. At the standard hair loss doses (dutasteride 0.5 mg vs finasteride 1 mg), scalp DHT suppression is roughly comparable — approximately 50% for both.
This is genuinely counterintuitive given the dramatic serum DHT difference, and it deserves explanation. Dutasteride is extremely lipophilic and binds tightly to plasma proteins, which limits how much of the drug actually reaches scalp tissue. Even though it's a more potent enzyme inhibitor that blocks both isoforms, its tissue penetration into the scalp is poor enough that local DHT suppression is similar to finasteride at standard dosing.
So why is dutasteride clinically superior in head-to-head trials? Several factors probably contribute beyond raw scalp DHT numbers: a much longer half-life (5 weeks vs 6-8 hours for finasteride) provides more consistent suppression with fewer trough periods; Type 1 inhibition affects sebaceous gland DHT generation, which may bathe follicles separately from what gets captured in bulk scalp tissue measurements; and the drug distributes differently within scalp tissue compartments. The clinical superiority is real and well-documented — the trial data is clear that dutasteride produces better hair count outcomes than finasteride. The simple "more DHT suppression equals more hair" model just doesn't fully explain why.
The trade-offs with dutasteride are also real. Sexual side effects occur in approximately 4% of patients (compared to about 2% with finasteride). The 5-week half-life means side effects, when they occur, take much longer to resolve after discontinuation than with finasteride. Fertility effects on semen parameters have been documented, which matters for men planning to have children. Post-finasteride syndrome concerns, while controversial in their incidence, are amplified with dutasteride simply because the drug stays in the system longer.
For patients comfortable with these trade-offs who want the most-studied path to better outcomes, switching to dutasteride is reasonable and supported by strong evidence.
Option two: adding topical clascoterone
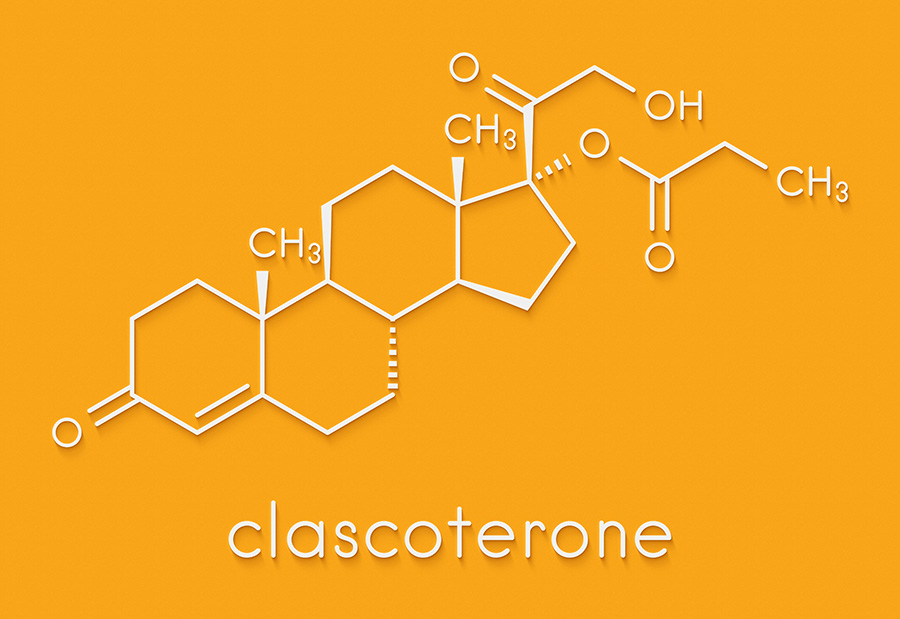
Clascoterone is a topical androgen receptor antagonist, FDA-approved in 2020 for acne under the brand name Winlevi. It works through a fundamentally different mechanism than finasteride or dutasteride. Rather than reducing DHT levels, it blocks the androgen receptor itself — the protein that DHT binds to in order to send the signal that drives hair follicle miniaturization.
The biology here is worth understanding. Hair loss happens when DHT binds to androgen receptors on susceptible follicles and initiates a cascade of changes — shortened growth phase, smaller dermal papilla, thinner hair shafts. 5-alpha reductase inhibitors like finasteride and dutasteride attack this by reducing how much DHT is available to bind. Clascoterone attacks it differently: even if DHT is present at normal levels, if the receptor is occupied by clascoterone, the signal doesn't get through.
This is the same principle that
combined androgen blockade — using both a 5-alpha reductase inhibitor and an androgen receptor antagonist — more effective than maximal 5-alpha reductase inhibition alone in prostate cancer treatment. You can't reduce DHT to zero, but you can substantially reduce signaling by attacking the pathway at two different points.
Clascoterone has a critical safety feature: it's rapidly hydrolyzed to inactive cortexolone by enzymes in the skin. This means that even though it's a potent androgen receptor antagonist, almost none of the active drug reaches systemic circulation. Sexual side effects, fertility concerns, and the prolonged drug residence time that comes with oral 5-alpha reductase inhibitors all become essentially non-issues with clascoterone. The drug is designed to work locally and stay there.
The Cassiopea Phase 2 trial of clascoterone in male androgenetic alopecia showed hair count improvements comparable to topical minoxidil 5% — a meaningful effect for a monotherapy. The trial used 5-7.5% clascoterone applied twice daily, higher concentrations than the 1% commercial formulation for acne.
The honest limitation: there is no published clinical trial evaluating the addition of topical clascoterone to oral finasteride. The combination we're discussing has never been formally studied. The argument for it is based on mechanism — attacking androgen signaling from two different points should produce more total suppression than attacking from one point harder — but the empirical evidence in this specific combination doesn't yet exist.
How the comparison actually shapes up
For a patient already on finasteride 1 mg who wants to go further, both options have real merit.
Switching to dutasteride brings stronger evidence and modestly more aggressive DHT suppression overall, accepting that at the scalp specifically the difference is smaller than the serum data suggests. The trade-off is meaningfully higher systemic exposure to a long-acting 5-alpha reductase inhibitor, with the associated side effect concerns.

Adding topical clascoterone provides a mechanistically distinct approach to the same biological pathway, with theoretical advantages in total signaling suppression and a dramatically improved systemic safety profile. The trade-off is weaker evidence — specifically, no trials of this combination — even though the mechanism is well-established in related contexts.
The choice between them depends on what the individual patient values. A patient who has been on finasteride without side effects and wants the strongest evidence-based escalation will likely choose dutasteride. A patient with concerns about future fertility, who has been hesitant about dutasteride for those reasons, or who has experienced side effects with oral 5-alpha reductase inhibitors and wants to minimize systemic exposure, may find the clascoterone option more aligned with their priorities. Both are defensible decisions.
For some patients, the right answer is to do both — continue finasteride or transition to dutasteride and add topical clascoterone on top, attacking the pathway at multiple points. This is the maximum medical therapy approach for committed patients who have plateaued on conventional therapy and want to push further.
What this means for treatment planning
The traditional treatment paradigm for androgenetic alopecia presented a fairly linear escalation: start with finasteride, switch to dutasteride if more was needed, then consider procedural interventions. The availability of topical clascoterone — alongside recent developments in oral minoxidil, topical 5-alpha reductase inhibitors, and combined formulations — has considerably expanded the medical therapy toolbox.
 At HMI, we don't recommend the same protocol for every patient. The right combination depends on the individual's response to current therapy, side effect tolerance, life stage considerations like family planning, and how aggressive they want to be. For most patients on finasteride who want to do more, the conversation about next steps now includes both dutasteride and clascoterone as legitimate options, with the recommendation tailored to their specific situation.
At HMI, we don't recommend the same protocol for every patient. The right combination depends on the individual's response to current therapy, side effect tolerance, life stage considerations like family planning, and how aggressive they want to be. For most patients on finasteride who want to do more, the conversation about next steps now includes both dutasteride and clascoterone as legitimate options, with the recommendation tailored to their specific situation.
The conversation that should happen with every patient considering escalation is honest: here's what we know about each option, here's where the evidence is strong and where it's preliminary, here's how each affects you systemically, and here's what realistic improvement looks like with each. Patients deserve to participate in this decision with full information rather than being handed a default protocol.
If you're currently on finasteride and considering what comes next, this is exactly the kind of decision a thorough consultation should walk through with you in detail.
Two options for going beyond finasteride alone.
For patients with a partial response on finasteride 1mg
Currently on finasteride 1mg
Serum DHT ~ 70% reduced
Scalp DHT ~50% reduced
Estimated functional androgen signal
at the follicle*
Estimated functional androgen signal
at the follicle*

*Receptor occupancy and functional signal estimates are theoretical, based on competitive antagonism principles and limited human data.